Transcription
Bosco et al. BMC Urology EARCH ARTICLEOpen AccessClinical and morphological effects ofhyperbaric oxygen therapy in patients withinterstitial cystitis associated withfibromyalgiaGerardo Bosco1, Edoardo Ostardo2, Alex Rizzato1, Giacomo Garetto3, Matteo Paganini1* , Giorgio Melloni4,Giampiero Giron5, Lodovico Pietrosanti5, Ivo Martinelli5 and Enrico Camporesi6AbstractBackground: Interstitial Cystitis (IC) is a debilitating disorder of the bladder, with a multifactorial and poorlyunderstood origin dealing with microcirculation repeated damages. Also Fibromyalgia (FM) is a persistent disorderwhose etiology is not completely explained, and its theorized alteration of pain processing can compromise thequality of life. Both these conditions have a high incidence of conventional therapeutic failure, but recent literaturesuggests a significant beneficial response to Hyperbaric Oxygen Therapy (HBOT). With this study, this study weevaluated the effects of HBOT on quality of life, symptoms, urodynamic parameters, and cystoscopic examination ofpatients suffering from both IC and FM.Methods: We structured an observational clinical trial design with repeated measures (questionnaires, urodynamictest, and cystoscopy) conducted before and 6 months after a therapeutic protocol with hyperbaric oxygen for thetreatment of patients suffering from both IC and FM. Patients were exposed to breathing 100% oxygen at 2 atmabsolute (ATA) in a multiplace pressure chamber for 90 min using an oro-nasal mask. Patients undertook a cycle of20 sessions for 5 days per week, and a second cycle of 20 sessions after 1 week of suspension.Results: Twelve patients completed the protocol. Changes after HBOT were not significant, except forhydrodistension tolerance (mean pre-treatment: 409.2 ml; mean post-treatment: 489.2 ml; p 0.05). A regression ofpetechiae and Hunner’s ulcers was also noted 6 months after the completion of HBOT.Conclusions: Our study showed no improvement of symptoms, quality of life, and urodynamic parameters, exceptfor hydrodistension, and a slight improvement in cystoscopic pattern. However, to date, we could not demonstratethe significance of overall results to justify the use of HBOT alone in patients with IC and FM. This observationsuggests that additional studies are needed to better understand if HBOT could treat this subset of patients.Trial registration: NCT03693001; October 2. Retrospectively registered.Keywords: Hyperbaric medicine, Interstitial cystitis, Fibromyalgia* Correspondence: and Respiratory Physiology Laboratory, Department ofBiomedical Sciences, University of Padova, Padova, ItalyFull list of author information is available at the end of the article The Author(s). Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License, which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication o/1.0/) applies to the data made available in this article, unless otherwise stated.
Bosco et al. BMC Urology 19:108BackgroundInterstitial Cystitis (IC) is a rare, chronic, and disablingcondition of the bladder that mainly affects females [1–3].The specific etiology of IC is currently unknown but seemsmultifactorial, with interactions among autoimmune, neuroendocrine, allergic, and infectious pathways [4, 5]. Theories suggested that IC could derive from an abnormallyincreased number of mast cells, or could be related to analteration of the glycosaminoglycan layer protectingurothelium from urine [6]. The activation of the inflammatory response induces alterations in the deep layers of bladder, such as fibrous substitution of the muscular tunic,thinning and discontinuity of the mucosa layer, capillaryproliferation, and blood vessel degeneration [7].Initial presentation of IC is subtle. The possible presenceof infection (due to urothelium damage), an increase in voidfrequency, and a pain resistant to analgesia are early symptoms that make the diagnosis more challenging because ofoverlapping with those present in bacterial cystitis and several other diseases [8]. Unfortunately, patients spend about 5to 10 years and a mean of 8 consults from different specialists before a correct diagnosis [9], while recurrent inflammation results in scar tissue development. The subsequentreduction of both bladder compliance and capacity, in conjunction with the gradual loss of functionality, determinechronic urinary tract symptoms [10], thus prompting cystoscopy and urometry that finally make the late diagnosis. Sincethe primary cause of IC is still hypothesized, conventionaltreatments – such as physical therapy, antidepressants, pentosan sulfate, immunosuppressants, intravescical therapywith lidocaine heparin and bicarbonate, and surgery [11] –mainly aim to alleviate symptoms. The effectiveness of mosttreatments does not exceed 60%, and symptoms return evenafter a period of improvement or recovery [9].A pilot study showed that 76% of patients with histologically confirmed IC have another medical condition, such asFibromyalgia Syndrome (FM), Chronic Fatigue Syndrome,and Irritable Bowel Syndrome [12]. FM is a persistent anddebilitating disorder that compromises the quality of life, affecting 2–4% of the population with a 9:1 female to maleratio [13]. There is no agreement on the specific etiology ofFM, even if some authors suggest that an abnormal brainactivity regarding pain processing could be the leadingcause [13]. Patients suffering from FM typically presentwith a triad of widespread chronic pain of long duration ( 3 months), sleep disturbance, and fatigue. Nonetheless, thepossible association with other key symptoms such as allodynia, hyperalgesia, general muscular tension, nerve pain,cognitive impairment, and mood disturbance makes thediagnosis quite challenging because of several overlaps withother rheumatologic conditions [13, 14]. All these symptoms are included Fibromyalgia DiagnosticCriteria published by the American College of Rheumatology [15, 16].Page 2 of 7Several integrated programs were proposed for FM,mainly targeting symptoms management using bothpharmacological and physical exercise or behavioraltherapy, but there is no consensus about these treatments, that have still limited effectiveness [13].Recently, an increasing amount of literature suggestedthe efficacy of Hyperbaric Oxygen Therapy (HBOT) inpatients with IC or FM. For instance, van Ophoven and colleagues reported an improvement of symptoms and bladdercapacity in patients affected by IC and treated with HBOT[5], results confirmed also by Tanaka in patients with aform of IC resistant to conventional therapy [4]. On theother side, Yildiz and colleagues found a significant reduction of Visual Analogue Scale scores in patients affected byFM and a significant increase in pain threshold [17]. Moreover, the work of Efrati and colleagues demonstrated a decrease in symptoms of FM and positive changes in brainactivity [13], concluding that HBOT plays an important rolein FM management. However, no study has investigatedthe possible role of HBOT in patients affected from ICassociated with FM (IC/FM) so far.The aim of our study was to investigate the response ofIC/FM patients subjected to HBOT. In detail, we evaluatedthe effectiveness of HBOT in IC/FM refractory to conventional therapy, focusing on changes in quality of life, painmodulation, modifications in bladder endoscopic and urometric patterns.MethodsSubjectsPatients were enrolled and considered eligible for thestudy after a medical screening carried out at the ATiPCenter of Hyperbaric Medicine (Padova, Italy), in order toexclude possible contraindications to HBOT (Fig. 1). Noincentives were offered to increase the enrollment andcompliance to the study. The inclusion criteria were: (a)pain in bladder filling that improves with urination; (b)pain (suprapubic, pelvic, urethral, vaginal, or perineal); (c)presence of glomerulation (grade II/III) (or bleeding / at the cystodistension) and positive histologic findings atbiopsy [18]; (d) reduced capacity; (e) increased visceralsensitivity; (f) normal or reduced compliance; (g) symptoms refractory to conventional therapy; and (h) diagnosisof FM according to the American College ofRheumatology guidelines [15, 16]. These criteria werebased on those of the European Society for the Study ofInterstitial Cystitis (ESSIC), including patients with anESSIC disease staging 2C [18].The exclusion criteria were: (a) pregnancy (diagnosed orwithin the previous year); (b) age less than 18 years; (c) benign or malignant bladder tumors; (d) radiation cystitis;(e) symptomatic bladder diversions; (f) herpes in activephase; (g) bladder and urethral stones; (h) urinary frequency less than 10 times a day; (i) presence of symptoms
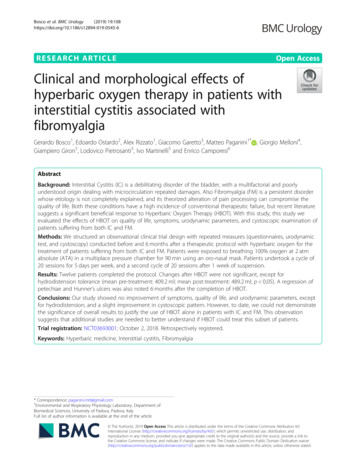
Bosco et al. BMC Urology 19:108Page 3 of 7Fig. 1 Flow-chart of experimental design. Eligibility and recruitment of patients. Details are reported in the textless than 12 months; and (l) bladder capacity 400 ml withno sensitive urgency.Experimental protocolThe experimental protocol received the approval by thelocal Human Ethical Committee (n HEC-DSB 07/16) ofthe Department of Biomedical Science at University ofPadova and adhered to the principles of the Declarationof Helsinki. Patients involved in the study read andsigned an informed consent, were free to renounce thestudy at any time, and every precaution was taken toprotect their privacy. All the patients were informedabout the methods and aims of the study.We structured an observational clinical trial design withrepeated measures conducted before and 6 months after atherapeutic protocol with hyperbaric oxygen for thetreatment of patients suffering from IC/FM. The authorsconfirmed that all ongoing and related trials for this intervention were retrospectively registered in the registry (NCT03693001). This study was not registeredbefore enrollment of participants started because IC is anapproved indication for HBOT in Italy and HBOT sessionswere already planned in the therapeutic schedule of the enrolled patients. The whole study, comprehensive of recruitment and follow up after the experiment, took placebetween January and September . This period seemedadequate for an evaluation over time of the treatment results on the most relevant symptoms of the pathology, i.e.pain, frequency of urination, urgency and evaluation ofbladder capacity [1, 5]. Patients were exposed to breathing100% oxygen at 2 atm absolute (ATA) in a multiplacepressure chamber (Galeazzi, Zingonia, Italy) for 90 minusing an overboard demand regulator while breathingthrough an oral-nasal mask. Each patient undertook a dailycycle of 20 sessions, 5 days a week. After 1 week of suspension, a second identical cycle of 20 sessions was performed.The primary outcome was the modification in symptoms, assessed through several questionnaires that wereadministered to patients before (PRE) and 6 months after(POST) HBOT: (a) three-day voiding diary, (b) widespread pain index (WPI), (c) symptom severity scale(SSS), (d) Pelvic pain, Urgency and Frequency symptomscale (PUF), and (e) O’Leary-Sant questionnaire.QuestionnairesThree-day voiding diaryIt is a sheet for each 24-h period. Patients specified theirbedtime and wake-up time directly in the upper part of thesheet. Later, they started recording all fluid intake (i.e., thetotal amount of fluids drank during a given time period)and urinary events (i.e., the amount of urine voided eachtime over a 24-h period). Moreover, the voiding diary presents specific fields to indicate either the amount of urinedrained via catheter and/or each time the pad was changed.Patients write each time they had involuntary urine loss(even a small amount). As final outcomes, mean and maximum urine volume were considered.Widespread pain indexWPI is a clinical diagnostic criterion proposed for patients with FM that do not rely on counting tenderpoints [15]. It considers not only pain but also other
Bosco et al. BMC Urology 19:108Page 4 of 7FM-related symptoms assessing their severity [15]. Physician asked the patient to indicate the location of anypain experienced during the week before the exam. As aresult, WPI pointed out a total amount ranging from 0to 19 points corresponding to the possibly-painful 19body areas (i.e., areas of the shoulders, arms, hips, legs,jaws, chest, abdomen, back, and neck) [14].Urodynamic testing allows recording of bladder sensitivity, capacity, and compliance as well as urethral and detrusor activity during filling. PRE and POST cystoscopy,hydrodistension, and urodynamic testing were performed by the same urologist, and urodynamic evaluation followed current International Continence Societystandards.Symptom severity scaleStatistical analysisSSS focuses on 3 physical symptoms, as well as somaticsymptoms in general [16]. In detail, symptoms are measured on the basis of a 0–3 severity scale consideringfatigue, waking unrefreshed, and cognitive symptoms. Theinvestigated period is the week before the questionnaire administration [14]. Later, the items are combined into a 0–12 scale assessing the somatic symptoms in general. Thegreater the amount, the more severe the symptomatology.Data were coded on a master sheet using a LibreOfficeCalc spreadsheet (ver. 6.0.1.1, The Document Foundation, Berlin, Germany). A Two-tailed t-test fordependent means was used to analyze differences between pre and post-treatment means of questionnairesand quantitative data from Urodynamic testing, with asignificance level of .05. Qualita